
From the 1Department of Neurological Physiotherapy, 2Department of Pediatric and Neonatal Physiotherapy, Maharishi Markandeshwar Institute of Physiotherapy and Rehabilitation, Maharishi Markandeshwar (Deemed to be University), Mullana-133207, Ambala District, Haryana, India.
E-mail: asirjohnsamuel@mmumullana.org
The World Health Organization (WHO) report that the safest method to prevent coronavirus 2019 (COVID-19) infection is through social distancing and social isolation (1). However, this poses various challenges for healthcare workers and patients, regarding the provision of rehabilitation services during COVID-19 lockdowns. Neurorehabilitation professionals are at high risk of exposure to COVID-19 due to close proximity with patients. Many neurological patients require regular rehabilitation services in order to improve their outcomes and quality of life, and these may be affected by social distancing (2).
Digital provision via the internet and other tools can provide new possibilities in care provision and follow-up for patients with neurological and related disorders. The application of information and communication technologies (ICT) in healthcare settings is termed “e-health”, and can help patients achieve goals in activities of daily living, improve their lifestyle, and to provide care, follow-up and intervention opportunities that are accessible to all individuals at the community level. Mobile-based rehabilitation (MBR) uses technology for communication between therapists, patients and caregivers (2). Everyday technologies have become an integral component of rehabilitation. Mobile devices, such as smart-phones and tablets, can be used as assistive equipment to improve individuals’ functional performance. MBR equipment comprises web-based devices and internet connectivity for the therapist and in the patient’s home.
Mobile-based health apps are promising tools for use in healthcare. Advanced technologies are being developed to increase patient participation and reduce disability. The use of mobile device based apps has been the focus of several recent clinical practices in neurological rehabilitation (3).
MBR provides an alternative means of delivering rehabilitation services to remote areas or to patients who are unable to visit hospital/clinics on a regular basis. It can be used to support rehabilitation services and help to prevent decline, to diagnose, and to provide therapeutic care. MBR may be an accessible method of providing rehabilitation care during social distancing. Consultation via video-conferencing can help to keep patients safe and prevent infection, although if patients need urgent hospital care full preventive measures should taken (4). Rehabilitation team members must be educated in the correct use of personal protective equipment (PPE) and infection control procedures.
MBR can help patients to continue their exercise protocols through the use of exercise videos. In order to minimize connectivity problems videos of exercises can be provided to the patient in advance and professionals can guide the patient using real-time instructions via video conferencing (5). The provision of 20 min of stretching, strengthening and balancing exercises in each session, guided by rehabilitation professionals using video-conferencing, may be beneficial in min-imizing overall decline in functional status during lockdown due to COVID-19 (6).
The authors recommend providing WhatsApp video-based rehabilitation and consultation to groups of patients, together with monitoring and guidance. Online video-based group therapy enables patients to communicate via audio, text or video messaging. A WhatsApp group video-conferencing call can currently include up to 8 people; hence it can be an effective and feasible means of providing group therapy to a number of patients on a single platform. Other web-based platforms can be used to provide group therapy to large numbers of people via video-based rehabilitation or consultation, e.g. Google Duo, Google Meet, Microsoft Teams, WebEx and Zoom.
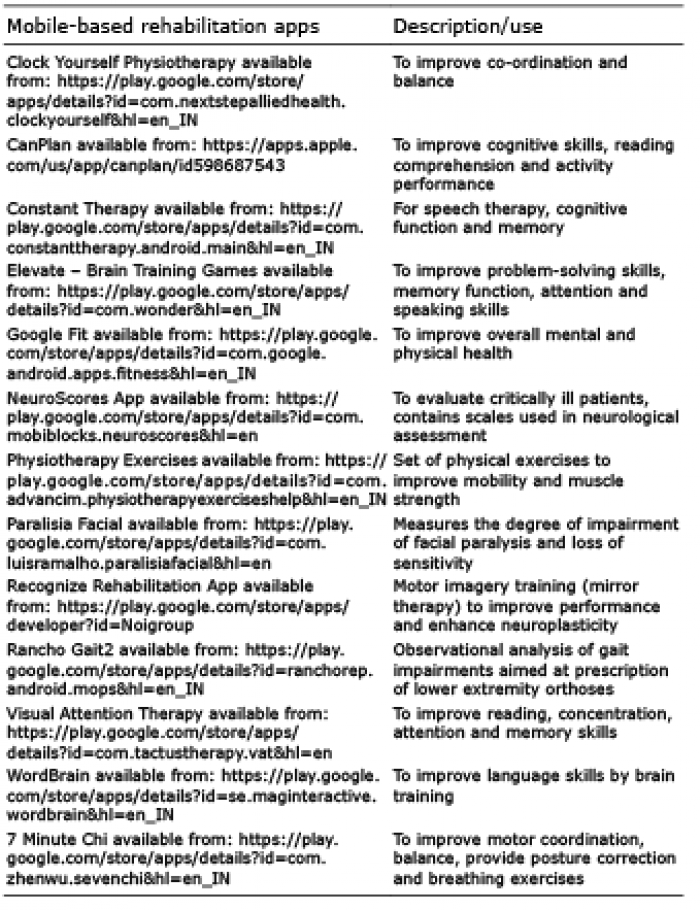
Various mobile-based apps that may be used in the rehabilitation of neurological patients during the COVID-19 pandemic are listed in Table I. Various aspects of rehabilitation can be provided via MBR, e.g. healthcare monitoring, providing therapy, education and functional assessments. The advantages and disadvantages of MBR are listed in Table II.
Accepted Aug 25, 2020; Epub ahead of print Sep 3, 2020
J Rehabil Med 2020; 52: jrm00099
Table I. Mobile phone based applications for use in e-neurorehabilitation
Table II. Advantages and disadvantages of mobile-based rehabilitation (MBR)
During social distancing inadequate access to rehabil-itation may occur in both rural and urban community areas. Rehabilitation professionals may be able to assess the home environment via videoconferencing and advise on the modifications needed for rehabilitation. Mobile-based apps can benefit healthcare professionals and increase patient access to point-of-care. MBR assists professionals to monitor and manage the patients’ condition, make clinical decisions and access health-
related training. In the current pandemic, the use of MBR should be explored to provide neurorehabilitation to all levels of the community and to improve the impact on functional and patient-centred outcomes. Use of MBR could increase accessibility to neurorehabilitation in remote areas, where provision of rehabilitation services is challenging, relieve the burden on current traditional healthcare systems and provide more effective use of digital resources to improve patient outcomes.
This letter was submitted as an assignment by the first author to the second author (mentor) as a part of University Research Fellowship (URF) programme during COVID-19 lockdown.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize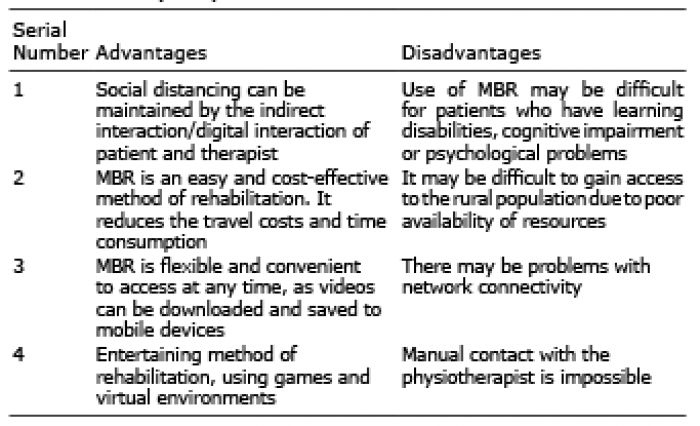 Click to show fullsize
Click to show fullsize